Ceramic Implant

Ceramic implants are dental implants made of a ceramic material that are shaped like a small screw. They are inserted into the jawbone of the tooth gap and are used to replace a lost tooth.
Ceramic implants show excellent health compatibility, adapt to the gums and jawbone ideally, and set new standards in terms of aesthetics.
In this article, we would like to provide our patients with a detailed insight into the topic of ceramic implants.
Who are ceramic implants suitable for?
Ceramic implants are suitable for patients who are looking for a healthy and stable solution after a tooth extraction.
After tooth loss, ceramic implants are a valuable solution to close the gap between the teeth without harming one’s health. This is due to the ceramic material, which is biocompatible and very suitable for dental implants.
Ceramic also offers great aesthetics and is therefore also recommended for patients who want a natural tooth replacement.
Duration and procedure for placing a ceramic implant
Placing a ceramic implant takes about 30 minutes to a maximum of one hour. This depends on whether the tooth is extracted and the implant is placed immediately, or if there is already a gap between the teeth.
Before the ceramic implant is placed, the jawbone is prepared so that the implant screw can be inserted with a precise fit. The ceramic implant is then screwed into the jawbone. It is important to ensure that the axis, depth and torque are correct.
Ceramic implant placement can be combined with bone augmentation to increase long-term stability.
Ceramic implants require a healing time of approximately 3 months. During this time the bone is not yet fully connected to the implant, therefore little to no pressure should be put on the implant.
If implants are necessary in the front, the patient is given fixed provisional restorations made of composite, for aesthetics during the healing period.
After the ceramic implants have healed, individual ceramic crowns are cemented without a gap, after which the treatment is completed.
Ceramic implant advantages
Ceramic implants have several advantages that patients should know of if they are thinking about getting a dental implant. So, not only does it benefit one’s health, but also the dental aesthetics. The advantages of ceramic implants are listed below.
Zirconia is biocompatible
Ceramic implants are made of zirconium dioxide, a material with excellent health compatibility.
Due to its extreme low solubility in aqueous solutions and inertness, its biological properties are ideal.Gums love ceramics
Fewer bacterial biofilms and plaque accumulate on ceramic implants than on titanium implants. The surrounding gums adhere very well to ceramic and the risk of gingivitis is significantly reduced (Rimondini et. al 2006). Ceramic implants are even less prone to gingivitis than natural teeth (Blaschke, Volz, 2006).
The adjacent gingiva shows very good blood circulation and forms a strong bond with the ceramic. This gum-ceramic bond prevents the penetration of oral bacteria into the bone and thus into the blood circulation system. Therefore, the “immunological door” is closed, which is an important essential for health.
Consequently, there is less inflammation around the implant, which speaks for the high long-term success of ceramic implants.
Integration into the bone
In addition to the excellent attachment of gums, the jawbone can adapt very well to the ceramic implants and be integrated by the jawbone. This good osseointegration has been proven in many studies. After only a few minutes, an accumulation of fibrin forms on the ceramic surface. The formation of such a fibrin network is the prerequisite for optimal healing in the bone.
Ceramic is rigid and does not deform
Since the entire ceramic implant does not deform due to masticatory forces, it remains rigid and immobile.
The lack of movement and deflection means that there are no pressure peaks on the surrounding bone, thus preserving the existing bone height.Ceramic can be customized
The abutment (implant abutment) is cemented onto the ceramic implant, completely gap-free. Then both the ceramic implant and ceramic abutment can be individually milled as a preparation for the ceramic crown. Here, the procedure is exactly the same as for a natural tooth. This is a great advantage because the crown margin can be perfectly adapted to the gum. Grinding the ceramic does not reduce the stability of the material. This has been confirmed in recent studies.
Excellent esthetics
Ceramic implants are white, which is a considerable advantage for natural aesthetics and beautiful teeth.
This is because, should the gums recede somewhat, the visible white margin is not obvious, but blends in visually with the overall appearance.
A metallic grayish color, on the other hand, as with titanium implants, does not look aesthetic or healthy.
Ceramic implant disadvantages
Ceramic implants also have some disadvantages, which patients should know before making a decision. The disadvantages of ceramic implants are listed below.
Ceramic implants can break
Ceramic implants are harder than titanium dental implants, but they can break when subjected to extreme pressure. Titanium, on the other hand, does not fracture but can bend. With the latest generation of ceramic implants, however, the likelihood of fracture is negligible.
Longer healing with old ceramic implant systems
In the past, ceramic implants took longer to heal. With today’s ceramic materials and implantation techniques, ceramic implants heal just as quickly as titanium implants. Depending on the situation and implant system, the patient should wait a minimum of three months before putting any pressure onto the implant.
Ceramic implants require dentists to rethink
Handling of ceramic implants is different than with titanium implants in many aspects, which requires dentists to rethink implantology. For example, the tissue reacts differently to ceramic, heat is dissipated differently, and many points must also be taken into account when preparing the bone.
Ceramic implants do not heal under local inflammation
Ceramic implants have the characteristic of not healing if there is inflammation in the bone or gums. Thus, a ceramic implant will only heal if the jaw inflammation is thoroughly cleaned after tooth removal. In addition, before the implant is placed, the wound should be disinfected, e.g. with ozone.
Risk of overheating the bone
Since ceramic is not able to dissipate heat as well as titanium, great care should be taken to not overheat the bone when inserting the implant. An implant may not heal if the bone has been subject to overheating.
Higher costs
The overall cost of ceramic implants is higher than titanium implants. This is because the manufacturing process is very expensive. Also, there are more steps to consider when placing ceramic implants, compared to titanium implants.
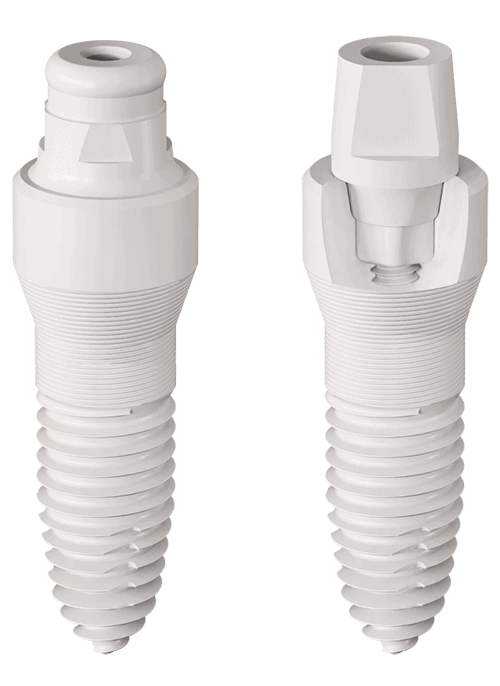
Shape and structure of a ceramic implant
In addition to the biological and physical properties of the materials, the shape of the implants is also of great importance. A distinction is made between one-piece and two-piece ceramic implants.
One-piece ceramic implants consist of one complete piece and combine implant body and implant abutment. These mainly replace anterior teeth and are less frequently found in the posterior region.
Two-piece ceramic implants have an implant body, which is the actual screw, and a separate abutment. After the implant has healed, these two components are bonded together with a cement so it is fixed and immovable.
Experience with ceramic implants
Nowadays, the use of ceramic implants in dentistry is more common and steadily increasing. The first ceramic implant was introduced in 1967 by the dentist Professor Sami Sandhaus. At that time, the material used was aluminum oxide, which had an insufficient prognosis and consequently could not establish itself in implantology.
Meanwhile, ceramic implants are now advanced and optimized, so that success rates have risen to 98%.
SDS implants are currently the most commonly used ceramic implants and have some advantages as immediate implants.
However, there are other implant companies that are bringing innovative ceramic implants to the market. For example, Zirkon Medical’s PATENT ceramic implant has many advantages in terms of healing and stability.
Our dentists use both SDS implants and PATENT implants, depending on the individual situation of the patient.
Ceramic implants cost
The costs of ceramic implants are higher than titanium implants, which should be considered by patients before making a decision. The reasons why ceramic implants are more expensive than titanium implants are as follows:
- Expensive manufacturing costs and therefore a higher selling price to the end user.
- More steps need to be followed in placing the ceramic implants to ensure an ideal result.
The exact implant cost can only be determined after a thorough examination in the dental practice.
Possible alternatives to ceramic implants
The best or most ideal restoration for a tooth gap must always be decided on an individual basis. As a rule, a ceramic implant offers the most advantages and is clearly superior to any other tooth replacement. However, there are situations where a different tooth restoration can make more sense.
Ceramic bridge
A ceramic bridge connects two teeth that have a gap inbetween, and also provides a fixed prosthesis. For this, the respective teeth must be ground to form tooth stumps. The bridge is cemented onto these tooth stumps, which closes the gap in the row of teeth. The necessary grinding of teeth is the main disadvantage of this method.
Closing the gap with aligners or braces
Closing a gap with aligners or braces is also a possible alternative. However, this is a lengthy process and only makes sense in certain situations.
Leaving the gap
Leaving the tooth gap is also an option for some patients. However, it can cause neighboring teeth to tilt into the gap and teeth of the opposing jaw to grow into the gap. In addition, there is always bone loss in the corresponding region, which makes subsequent implantation more difficult and may require bone augmentation/grafting.
Denture
A denture is another alternative treatment of a gap. Despite the low cost, dentures have many disadvantages. The feeling of a foreign body, pressure points on the mucosa and visible bracket margins can be no-gos for the patient.
Dr. Josephine Phillips
A ceramic implant is an excellent solution for a lost tooth. Our experienced team is here to help.

Frequently asked Questions about Ceramic Implants
Below you will find the most frequently asked questions about ceramic implants. We will do our best to answer all important questions. If you have any unanswered questions, please feel free to contact us.
Many people wonder whether to choose a ceramic or titanium implant.
A ceramic implant has significant advantages over a titanium implant in terms of health and aesthetics. Read more in the article environmental dentistry.
Ceramic implants can also be used to replace molar teeth. For safe and successful results, it is important that the dentist/oral surgeon has a lot of experience with ceramic implants.
If the dentist has little experience with ceramic implants, it may occur that the upper part of the ceramic implant breaks off. Usually, this is a broken abutment (implant abutment), which can easily be repaired.
Although the production of implants is subject to the strict MDR (Medical Device Regulation), attention should always be paid to cleanliness when selecting an implant. Dental implants certified by Clean Implant are a good guide.
As long as the dentist knows how to place the implants ideally and how they are ground later after healing, the risk of fracture is not higher than with implants made of titanium.
Is the longevity of ceramic implants higher than that of titanium implants?
In our opinion, ceramic implants show much better longevity and better prognosis than titanium implants.
This is due to the following reasons:
- Ceramic implants show a very good, inflammation-free bond with bone and gums.
- Ceramic is clearly superior to titanium from a toxicological and allergological point of view (biocompatibility).
- Our implant systems are gap-free like a natural tooth, so there are no crevices where bacterial biofilms can form.
No, we only use ceramic implants made of zirconium oxide.
Depending on the situation, we use PATENT implants and SDS implants.
If a patient has received bisphosphonates in the past, jaw necrosis may occur after operations in the jawbone. This is known as Bisphosphonate-Induced Osteonecrosis of the Jaw (BRONJ) or Bisphosphonate-Related Osteonecrosis of the Jaw (BRONJ). This type of jaw necrosis is very dangerous and can result in needing to remove large parts of the jawbone.
Surgery should be avoided for patients who have received bisphosphonates in the form of injections (IV). In this case, placing dental implants is not possible. As for patients who have taken bisphosphonates in the form of tablets, the situation is reviewed individually.
Further information
The information listed contains relevant topics for a better understanding.